


Simulation training for EMS: Revolutionizing Prehospital Care
The prehospital environment is inherently chaotic, unpredictable, and entirely unforgiving. Unlike a brightly lit, temperature-controlled hospital operating room with a full team of specialists on standby, the streets, highways, and living rooms where emergency medical services operate present unique logistical and clinical challenges. In these high-stress environments, there is zero margin for error. Historically, prehospital providers learned their craft through a mix of classroom lectures and on-the-job clinical rotations. However, the modern paradigm of healthcare education demands a safer, more structured approach. Today, simulation training for EMS has emerged as the definitive standard for preparing first responders for the harsh realities of the field, ensuring they develop the critical thinking, psychomotor skills, and situational awareness required to save lives.

The Unique Challenges of Prehospital Medicine
To understand the necessity of advanced training methodologies, one must first understand the environment in which EMS professionals operate. When a 911 call is dispatched, paramedics do not know exactly what awaits them behind a closed door. They must bring the emergency room directly to the patient, often working in confined spaces, adverse weather conditions, and poorly lit areas.
Furthermore, EMS personnel often operate autonomously or in very small teams. A crew of two paramedics might be forced to manage a catastrophic multi-system trauma or a complex pediatric cardiac arrest entirely on their own for the first twenty minutes of a call. In these scenarios, a provider cannot pause to consult a textbook or wait for a senior physician to arrive. The required clinical interventions - such as rapid sequence intubation (RSI), intraosseous (IO) access, or needle decompression - must be executed flawlessly and immediately. This absolute need for autonomous perfection is exactly why a rigorous, simulation-based curriculum is non-negotiable.
Core Modalities of Simulation in EMS
The landscape of prehospital simulation encompasses a wide spectrum of tools, each tailored to specific educational objectives. A comprehensive EMS educational program will utilize a combination of these modalities to build a well-rounded practitioner.
Part-Task Trainers for Psychomotor Mastery
Before integrating complex decision-making, learners must master individual psychomotor tasks. Part-task trainers are anatomical models used to isolate and drill specific interventions. For example, airway management is a cornerstone of prehospital care. Using an intubation head simulator, paramedics can repetitively practice visualizing the vocal cords and passing an endotracheal tube until the muscle memory is firmly established. Similarly, intravenous (IV) arms and IO leg models allow trainees to practice gaining vascular access. By isolating these skills in a low-stress training environment, learners build the mechanical confidence necessary to perform them during a real crisis.
High-Fidelity Manikins
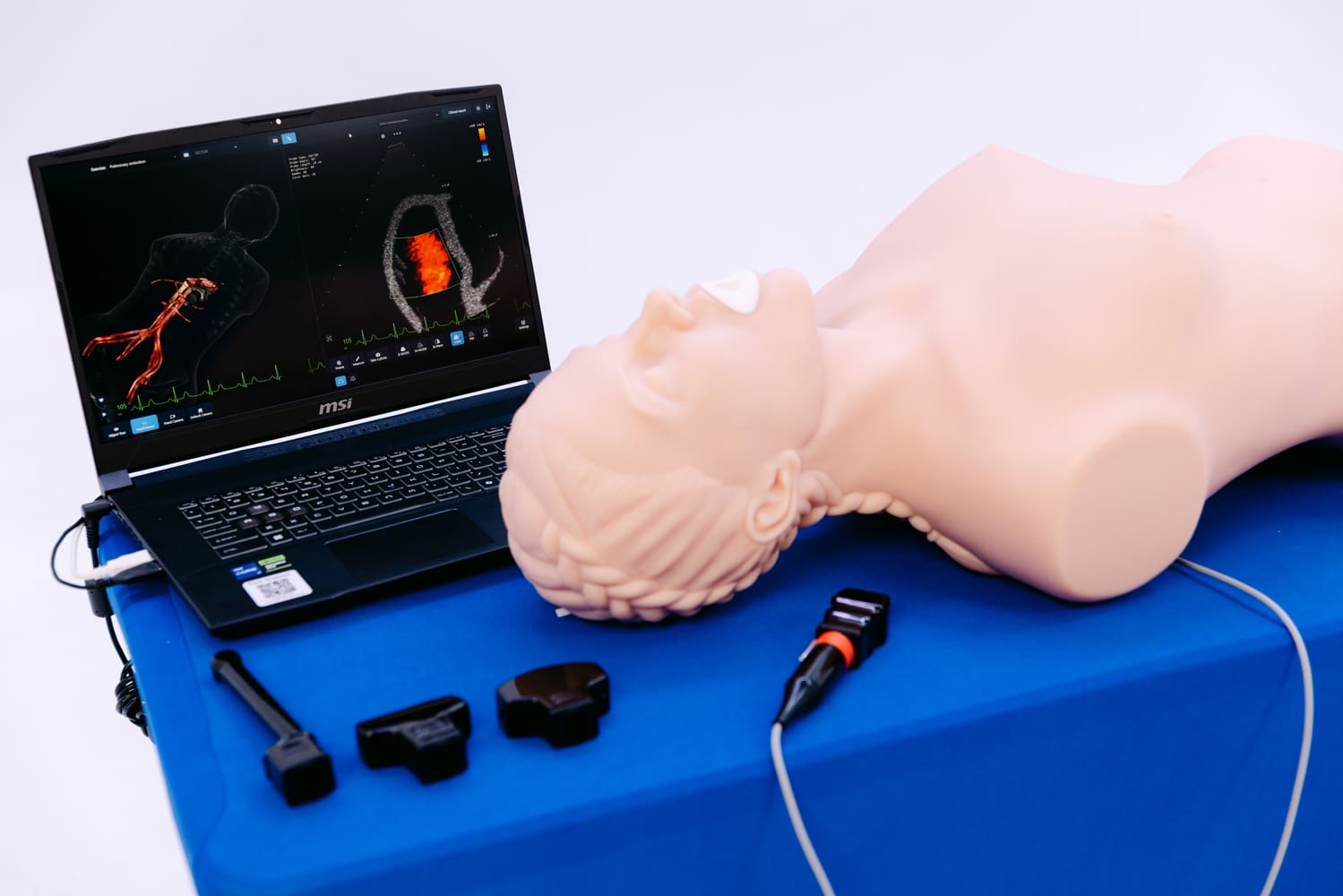
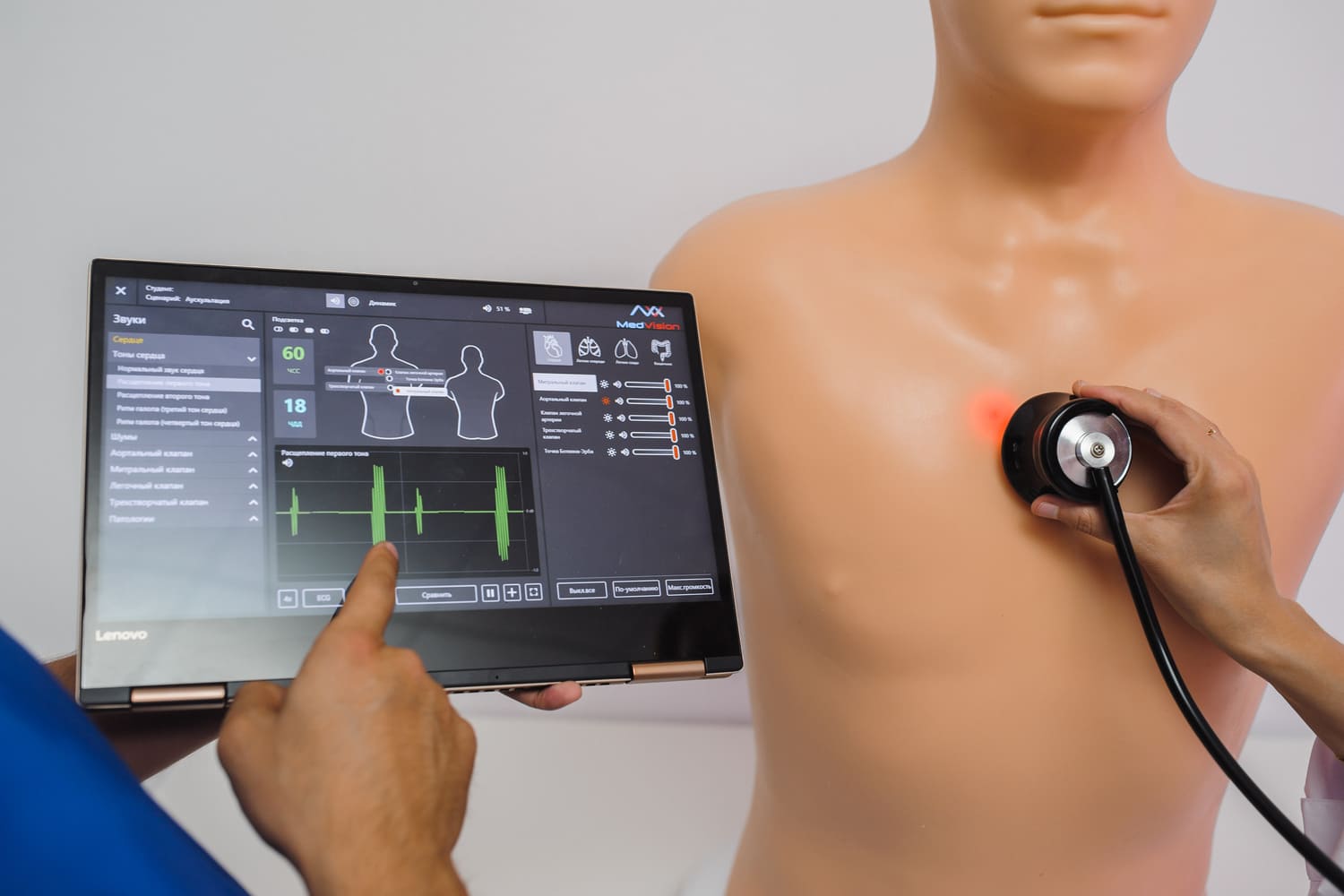
When institutions want to bridge the gap between mechanical repetition and true clinical reasoning, they turn to high-fidelity patient simulators. A modern, computerized simulator can perfectly replicate human physiology. These advanced manikins feature palpable pulses, reactive pupils, rising and falling chests, and the ability to produce realistic heart, lung, and bowel sounds.
Crucially, a high-fidelity simulator responds physiologically to the interventions performed by the paramedics. If a trainee administers the correct dose of epinephrine during a simulated anaphylaxis scenario, the manikin's vital signs will automatically improve on the monitor. If the wrong medication is given, the simulated patient will deteriorate. This dynamic feedback loop is essential for teaching pharmacology and advanced life support (ALS) algorithms.

Specialized Simulation Training for Paramedics
While Basic Life Support (BLS) providers focus on CPR and rapid transport, advanced providers require a significantly deeper level of clinical education. Simulation training for paramedics specifically targets complex, invasive procedures and advanced diagnostic interpretation.
One of the most critical areas of focus is 12-lead electrocardiogram (ECG) interpretation. Using a specialized simulator, instructors can generate complex cardiac arrhythmias, such as ventricular tachycardia or complete heart block. Paramedics must rapidly interpret the rhythm on their actual clinical monitors, determine the appropriate pharmacological or electrical intervention (such as synchronized cardioversion or pacing), and execute the treatment.
Another vital component of simulation training for paramedics is the management of High-Acuity, Low-Occurrence (HALO) events. These are catastrophic emergencies - such as pediatric cardiac arrest, complicated breech childbirth, or severe burn management - that are incredibly dangerous but happen infrequently in daily practice. Because paramedics rarely encounter these situations naturally, their skills can easily degrade over time. Routine training with a simulator is the only reliable method to ensure that providers maintain their competency and are ready to act instantly when a HALO event inevitably occurs.
In Situ Training: Bringing the Simulator to the Field
A major innovation in recent years is the transition from classroom-based laboratories to in situ simulation. In situ training involves physically moving the simulator into the actual working environment of the EMS crew - specifically, the back of a moving ambulance or an outdoor urban environment.
Practicing inside a moving ambulance introduces the authentic ergonomic challenges of the job. Paramedics must learn to establish airways, draw up medications, and perform chest compressions while balancing in a narrow, swaying compartment. By placing a high-fidelity simulator on a stretcher and running a scenario while the vehicle is being driven, educators can identify latent safety threats and workflow inefficiencies that would never be discovered in a stationary, spacious classroom. This environmental realism significantly enhances the psychological fidelity of the training.
Crew Resource Management and Team Dynamics
In the realm of emergency medicine, clinical knowledge is useless if it cannot be communicated effectively. Many adverse outcomes in prehospital care are not caused by a lack of medical knowledge, but by breakdowns in communication, leadership, and teamwork. Modern simulation programs heavily emphasize Crew Resource Management (CRM) - a concept originally adopted from the aviation industry to reduce human error.
During a complex simulation, educators assess how well paramedics assign roles, share mental models, and communicate using closed-loop communication techniques. For example, during a simulated multi-casualty incident, the primary challenge is not just treating the injuries, but effectively triaging multiple patients, managing limited resources, and coordinating with incoming fire department and police units. By practicing these complex team dynamics on a simulator, EMS agencies foster a culture of safety where every provider knows their role during a chaotic event.
The Critical Role of Debriefing
The actual time spent interacting with a simulator is only a fraction of the learning process. The true educational value of any simulation is unlocked during the debriefing phase. According to adult learning theories, reflective observation is where permanent cognitive change occurs.
After a training scenario concludes, the instructor and the paramedics gather in a safe, non-punitive environment to review the event. High-quality simulation centers utilize audio-video recording systems to review the team's performance minute by minute. During the debrief, the facilitator guides the EMS professionals to analyze their own clinical decision-making. Why was a specific airway adjunct chosen? How did the team react when the patient's blood pressure plummeted? By dissecting their thought processes and actions, paramedics identify their own knowledge gaps and solidify best practices. Without a structured debriefing, a simulation is merely an exercise in stress; with it, it becomes a profound educational milestone.

Conclusion
The delivery of exceptional prehospital care is not a matter of luck; it is the direct result of rigorous, uncompromising preparation. Simulation training for EMS has fundamentally shifted the educational paradigm from passive learning to active, experiential mastery. By utilizing part-task trainers, high-fidelity manikins, and in situ methodologies, agencies ensure that their personnel are exposed to every conceivable clinical challenge before they ever touch a real human being. For modern paramedics, the simulator is not just a training tool - it is an indispensable bridge between theoretical knowledge and life-saving clinical execution. As the demands on emergency medical services continue to grow, comprehensive simulation programs will remain the ultimate safeguard for both the provider and the public they serve.
References
- Alinier, G. (2011). Developing high-fidelity health care simulation scenarios: A guide for educators and professionals. Simulation & Gaming, 42(1), 9-26.
- Binstadt, E. S., Walls, R. M., White, B. A., Nadel, E. S., Takayesu, J. K., Barker, T. D., ... & Pozner, C. N. (2007). A comprehensive medical simulation education curriculum for emergency medicine residents. Annals of Emergency Medicine, 49(4), 495-504.
- Dieckmann, P., Gaba, D., & Rall, M. (2007). Deepening the theoretical foundations of patient simulation as social practice. Simulation in Healthcare, 2(3), 183-193.
- Lateef, F. (2010). Simulation-based learning: Just like the real thing. Journal of Emergencies, Trauma, and Shock, 3(4), 348-352.
- Lazzara, E. H., Benishek, L. E., Dietz, A. S., Salas, E., & Adriansen, D. J. (2014). Eight critical factors in creating and implementing a successful simulation program. The Joint Commission Journal on Quality and Patient Safety, 40(1), 21-29.
FAQ
Why is simulation training for EMS critical for patient safety?
The prehospital environment is unpredictable. Using a simulator allows providers to practice high-stakes, invasive interventions in a perfectly safe, controlled environment. This ensures that when an actual emergency occurs, providers have the muscle memory and clinical judgment necessary to act without causing harm.
What specific skills are focused on during simulation training for paramedics?
Advanced providers focus heavily on Advanced Life Support (ALS) procedures. This includes practicing rapid sequence intubation, intraosseous access, 12-lead ECG interpretation, and the administration of critical medications during simulated cardiac arrests or severe trauma scenarios.
How does a high-fidelity simulator differ from a standard CPR manikin in the training?
While a basic manikin is a static physical model used only for chest compressions, a high-fidelity simulator is a fully computerized system. It exhibits vital signs, pupillary responses, heart sounds, and reacts in real-time to the pharmacological and electrical interventions administered by the EMS team.
What is the role of debriefing in EMS simulation training?
Debriefing is the most crucial part of any simulation-based learning event. It is a guided, reflective discussion held immediately after the scenario. It allows paramedics to analyze their communication, teamwork, and clinical decision-making, transforming a practical exercise into long-term cognitive retention.
Immerse yourself in a demo to see how MedVision transforms traditional learning into an engaging, interactive experience

Subscribe for the Latest News!